Pretty sure a lot of us have been saying this since the beginning:
CNN medical analyst and Washington Post columnist Dr. Leana Wen admitted in a column, Friday, that the medical community is “overcounting” the amount of “COVID deaths and hospital…

nypost.com
Here is the original WaPo article. I don't have a sub, but for those who do:
The COVID overcounting should not really not a surprise to anyone- especially when there is no differentiation between deaths caused by COVID and deaths associated by COVID. This is especially true early in the pandemic when there was nothing resembling standardized reporting. What you consider to be a COVID death can be complicated when you have a patient with other comorbidities.
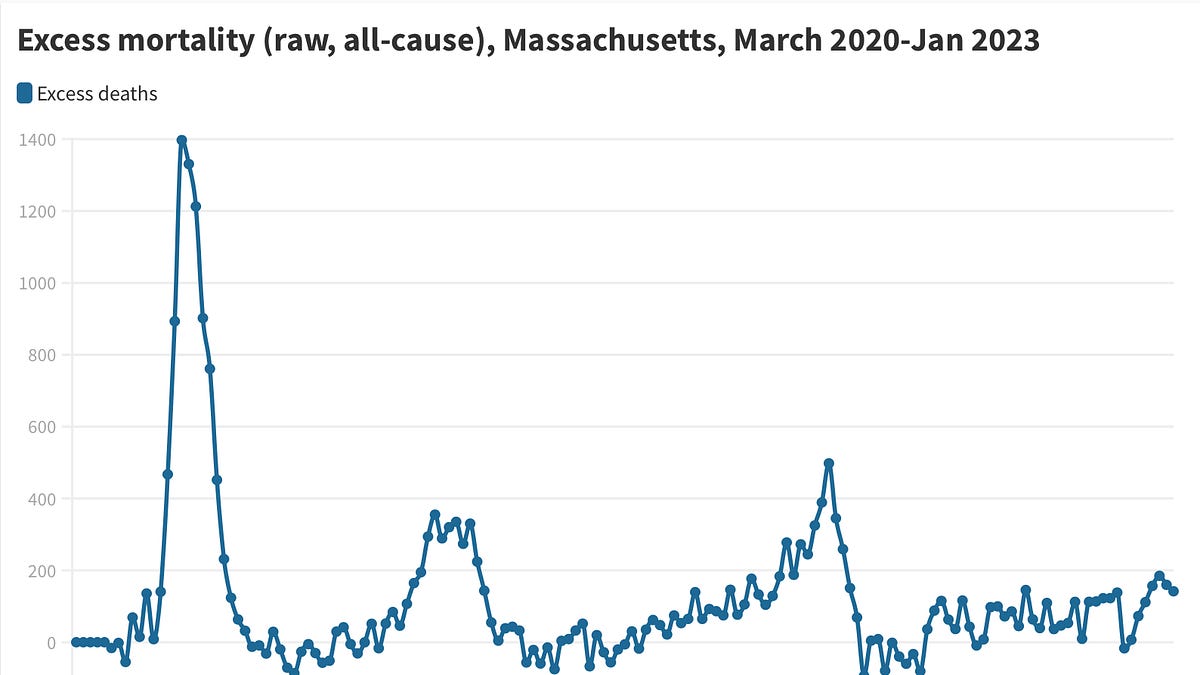
Here in Mass, less than a year ago, the state concluded they had overcounted COVID deaths by 15%- 4000+ deaths. Here’s how things worked here:
- 2020-2021- Anyone who died with a previous diagnosis of COVID was counted, even if they died in car accident from obvious trauma.
- 2021-2021- Anyone who had COVID within 60 days of dying was counted, unless the result of obvious trauma (ie car accidents not counted)
- **2022+ - Anyone who dies of COVID directly or where COVID contributes to death or who dies of “natural causes” within 30 days of COVID diagnosis (presumptive or lab confirmed Dx). It can also include family members who claim/believe the person died of COVID.
**The last bullet is (my paraphrased summary) of the
national standard for COVID reporting. I’m not sure if all states use the CSTE criteria, but many do. As you can see, there is a lot of wiggle room here.
I expect it will take years to sort this out these statistics, as often is the case with epidemics. And there will never be a definite figure.
COVID hospitalizations are also a mess because in many states, anyone hospitalized with COVID is counted as a COVID hospitalization. While the media often did not correctly report these numbers in the correct context, the general sentiment holds true- the more hospitalizations, the more cases among the population, and the more related deaths. I believe the CDC has now made it so only patients receiving treatment for severe COVID are reported.
The least accurate figure by far is the case count. Now that we have at-home rapid tests, there far less reporting on positive results. Most people aren’t going to upload their result per the mfg website or call their doctor to inform them unless they’re really not feeling well.
Over Xmas the state reported case counts around here were stable. But practically 1/3 of people I know got COVID during December… more than I’d ever seen at once. Deaths increased slightly which also suggests a rise. Wastewater virus levels skyrocketed. So I’d say our population-wide case reporting system is pretty useless at this point.
Epidemiology on pandemics/endemic diseases like COVID is tough to track. We’re never going to have anything close to an exact number, only a range of estimates.
Unfortunately any speak of COVID in the mass media either has some underlying political agenda or is interpreted to have one by people who have strong political opinions. I don’t have a WaPo subscription so I can’t make that assessment on the original article. But I don’t think it’s an unreasonable argument. For the sake of public argument though, I’m not quite sure why it matters at this point… aside for people comparing states’ fatality rates with no other variables considered to generate political commentary.
I’m very much over the toxic political BS that has destroyed public health.